COVID-19 doctors not allowed to use treatments that work - Dr McCullough Video and transcript May 2021


Table of contents
- Vimeo Video Interview 5/19/2021
- Introduction by John Leake
- Transcript
- He published The Pathophysiologic Rationale ,,,
- No positive feedback from his paper
- Emergency Use Authorization for hydroxychloroquine
- Fake paper published in Lancet
- Hydroxychloroquine - the most studied and used therapeutic
- Enormous effort to suppress early treatment. Hydroxychloroquine
- Hydroxychloroquin not cause scarring of the heart
- Hydroxychloroquin is useful, but not as a single drug
- ivermectin and FLCCC
- hydroxychloroquine and Ivermetic used for prevention and early treatment
- Drs. unable to get consensus when they could not meet during COVID-19
- His father got COVID-19 and was treated by zinc, vitamin C, vitamin D, quercetin, etc.
- our methods could reduce hospitalization and death by 85% - We're treating 10,000 to 15,000 patients a day.
- South Africa success customizing treatment to each patient
- 40% of drug use is "off label"
- Drs being told to not treat COVID-19 with drugs
- FDA, etc say what not to do, but does not say what to do
- monoclonal antibodies - emergency use authorized, big money, but no updated information
- Extensive "advertising" for vaccines, but nothing else
- monoclonal antibodies being squashed, vaccines promoted
- Vaccines were not tested on pregnant women, but they are vaccinated anyway
- Previous vaccines had 48 months of testing, this one had 2 months before getting EUA
- Feedback to his paper - do not try treating, we do not have published studies
- He and his wife got COVID-19 in October
- early treatment doctors started to become scrubbed
- America has offered nothing to the sick person.
- Early treatment without hospitals
- international Dr. group called C-19
- Combination therapy works, rarely wil a single drug work
- Drs. being penalized for prescribing treatments
- This is not new - The first Dr. using lung machine for polio was thrown off the staff
- Book: "COVID-19 and the Global Predators: We Are The Prey",
- Why are we vaccinating pregnancies, why are we vaccinating young health care workers?
- He had estimated maybe 20 million people would need to be vaccinated,
- We knew from the clinical trials that it didn't stop COVID-19
- He is pro-vaccine in general - but now 4,000 vaccine-related deaths
when Swine vaccine deaths reached 25, it was stopped - Marked in a database - but not if have nautral immunity?
- If the vaccine was like water ... who wouldn't take it?
- He had vaccinated many, but "I can no longer recommend it."
- - patients are getting vaccinated to something that doesn't even exist anymore
"It's just like giving everybody a narrow spectrum antibiotic" - Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection
- VitaminDWiki
- Mercola interviewed McCullough: video and transcript (before July 3, 2021)
- McCullough has weekly podcasts
- Presentation at Commonwealth Club in SF, July 14, 2021
- Rebutal
- Web
Vimeo Video Interview 5/19/2021
Dr. Peter McCullough Interview
Introduction by John Leake
Dr. Peter McCullough has been the world's most prominent and vocal advocate for early outpatient treatment of SARS-CoV-2 (COVID-19) Infection in order to prevent hospitalization and death. On May 19, 2021, I interviewed him about his efforts as a treating physician and researcher. From his unique vantage point, he has observed and documented a PROFOUNDLY DISTURBING POLICY RESPONSE to the pandemic — a policy response that may prove to be the greatest malpractice and malfeasance in the history of medicine and public health.
Dr. McCullough is an internist, cardiologist, epidemiologist, and Professor of Medicine at Texas A & M College of Medicine, Dallas, TX USA. Since the outset of the pandemic, Dr. McCullough has been a leader in the medical response to the COVID-19 disaster and has published "Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection" the first synthesis of sequenced multidrug treatment of ambulatory patients infected with SARS-CoV-2 in the American Journal of Medicine and subsequently updated in Reviews in Cardiovascular Medicine. He has 40 peer-reviewed publications on the infection and has commented extensively on the medical response to the COVID-19 crisis in TheHill and on FOX NEWS Channel. On November 19, 2020, Dr. McCullough testified in the US Senate Committee on Homeland Security and Governmental Affairs and throughout 2021 in the Texas Senate Committee on Health and Human Services, Colorado General Assembly, and New Hampshire Senate concerning many aspects of the pandemic response.
Peter A. McCullough, MD, MPH, FACP, FACC, FAHA, FCRSA, FCCP, FNKF, FNLA
Professor of Medicine, Texas A & M College of Medicine
Board Certified Internist and Cardiologist
President Cardiorenal Society of America
Editor-in-Chief, Reviews in Cardiovascular Medicine
Editor-in-Chief, Cardiorenal Medicine
Senior Associate Editor, American Journal of Cardiology
For more information about Dr. McCullough, please visit: heartplace.com/dr-peter-a-mcculloug
Transcript
0:00:11.2 Dr. Peter McCullough: I'm Dr. Peter McCullough, and I'm an internist and cardiologist, and academic physician, professor of medicine at Texas A&M College of Medicine on the Baylor, Dallas campus. And in February of 2020, like many physicians, I was really taken by storm with the news that a tremendously contagious virus was emanating out of Wuhan, China, and it looks like the United States was in the cross-hairs.
0:00:47.2 DM: In the beginning, in my clinical practice, I really didn't have any viewpoint about prior viral pandemics, and some had mentioned prior influenza, pandemics... We go back to 1300s, there was plagues that occurred across Europe, but point in fact, we were largely and very quickly thrown into emergency mode, and so what happened was a whole series of communications within health systems that really dealt with protection of the doctors and nurses and Americans were introduced to a term called PPE or personal protective equipment, and most of our task force meetings and calls really didn't have to do with sick patients, it had to do with protection of the health care workers and doctors, so I got a sense early on that fear, group fear was a major driver in behavioral response to the pandemic.
0:01:44.4 DM: My research endeavors and my research life before COVID-19 centered on the interface between heart and kidney disease, I'm the president of the Cardio Renal Society of America, I'm considered the most published person on this topic in the world in history, I chair many FDA approved clinical trial data safety monitoring board. In fact, I've probably seen and examined more drug safety trial data than any doctor in current American medicine, so I'm well-grounded in chronic disease epidemiology in randomized trials but for COVID-19, our major viewpoint that we had early on, or at least for me with my prior cardio renal collaborations was with Italian doctors, and so we were starting to email each other in terms of what is going on in the Metro Milan area, and Milan and then down to Siena and Tuscany, and we quickly started to get an understanding that this illness was like a upper respiratory infection, like a common cold, and for a majority of individuals, it was like the common cold, however, in some individuals, it could progress to what we call the Adult Respiratory Distress Syndrome, where there's an overwhelming attack against the lungs, patients lost their ability to breathe and exchange oxygen and carbon dioxide, and then required mechanical intubation, so this was unlike any common cold, and it appeared to be very different than influenza.
0:03:18.2 DM: Influenza in elderly people can also cause the Adult Respiratory Distress Syndrome, but it's almost always because of a secondary bacterial infection, like staphylococcal infection. So SARS-CoV-2, the virus in COVID-19 appeared to have these special features, and then within a few weeks, we understood pretty clearly that the illness had three major biological features to it, one was early viral replication where the virus replicates exponentially as other viral infections do. And that it has a second phase where the immune system is tipped off into a very abnormal maladaptive pattern, so instead of the immune system defending the body, the immune system sends out signals that begin to damage organs, including the heart, the lungs, kidneys, the brain, the blood system, and then very importantly, the virus itself, through the spike protein or the dangerous spicule on the surface of the ball of the virus, the spike protein itself caused coagulation or blood clotting and a unique type of coagulation. It caused the red blood cells to stick together at the same time, the platelets stick together, so this is a very different type of blood clotting that we would see with major blood clots in the arteries and veins, for instance, blood clots involved in stroke and heart attack, blood clots involved in major blood vessels and the legs.
0:04:50.1 DM: This was a different type of clotting, and in fact, the Italians courageously did some autopsies and found micro-blood clots in the lungs, and so we understood in the end, the reason why the lungs fail, it's not because the virus is there, it's because micro blood clots are there.
0:05:11.9 DM: The waves of reports and published medical literature originally emanated out of China, the early ones, and the public should understand that the typical publication cycle for an academic paper that's peer-reviewed and published can be anywhere from nine months to two years. So what happened was the publication cycles were too long to get any rapid information out, so immediately our system collapsed into what's called pre-prints, so publications would be submitted, papers would be submitted for publication, but the pre-print would come out basically telling the world that the paper had not yet undergone peer review, but we need to get this information out now 'cause people need to understand what's going on. So we had a wave from China originally, which was difficult to interpret because of English writing, because the Chinese population is just so different in terms of its structure, and it was hard to make much out of what was coming out of China outside of... In some cases, it could be fatal.
0:06:15.5 DM: Italy was much more like the United States, there was the next big wave, and we just collaborate more freely with the Italians, and what I had done is I had reached out to what's called the cortical network in Italy as an American doctor, and I freely said, Listen, I am not a virologist or an immunologist, but I can tell you every infectious disease doctor in America is completely subscribed to inpatient care of patients with COVID-19, and there's nobody able to think their way through what's going on in the pandemic. And so what we learned relatively early is that this illness was clearly and strongly amenable to risk stratification or that baseline risks were very, very strong determinants, even more so than the virus itself for mortality. So what that meant is the strongest determinant of mortality is age, and age itself is an underline determinant or a cause of death, if you will, in the general population, then we start adding on the typical things that put people at risk for death of other causes, heart disease, lung disease, kidney disease, cancer, obesity, diabetes. The interesting thing is that obesity appeared to be a super loaded factor, and so the virus seemed to really prey upon patients, particularly who are obese.
0:07:40.6 DM: And there are some reasons for this in terms of how the cytokines and immune factors are generated in response to the virus that could explain it, but we understood quickly that individuals under age 50, for example, with no major medical problems, could ride through this illness very easily, and in fact, the Swedes figured this out very quickly and said, You know what, we're not gonna shut down, we can just... This is sufficiently understood that we can simply protect the individuals at risk the best we can, the best that any protection measure can, and then we'll just have our economy and our schools move along in a usual fashion. With the pandemic, what happened is it was a global shutdown on travel and a global shutdown in academic meetings, so for the first time in my career, we could no longer meet with our colleagues in the United States or overseas. And academic medicine, its life blood is meeting an interchange of ideas. And so for the first time, we could not freely interchange ideas as a group.
0:08:46.6 DM: In fact, I recall a teleconference early on, held by the National Institutes of Health, strictly actually by the Division of insulin... Of Diabetes and Kidney disease, it was that institute that I'm aligned with in terms of clinical trials and it was led by Dr. Robert Star, a terrific scientist, and as I recall, there were hundreds of people on the call to just learn about what was going on in other centers, and people were asking each other, Well, what are you seeing out at UCLA? What are you seeing at Baylor? And what are you seeing at Harvard? And so we were literally just communicating to try to understand what in the world is going on with this virus? Who needs to be hospitalized? What happens when they're hospitalized? Who needs mechanical ventilation.
0:09:33.3 DM: All of these interactions had us settle on the idea that this was enormously amenable to risk stratification. People under age 50 without new medical problems, unless they presented with severe symptoms, they were gonna be fine, honestly, it was gonna be like a head cold. But over age 50, there became a real risk of hospitalization and death, and the two important endpoints, the two important endpoints were hospitalization and death. If you ask Americans, What are you afraid of? Are you're afraid of getting a cold and being at home for a few days or a few weeks? No, I'm afraid... I'm definitely afraid of being hospitalized and obviously afraid of dying. Why was the hospitalization so frightening? Because for the first time, patients would be hospitalized, they were put into isolation, they could never see their loved ones again.
0:10:21.6 DM: Those who died actually never did see their loved ones again. The workers were terrified, they were wearing personal protective equipment, they had very reduced visitation to patients in rooms, they started using telemedicine services were the poor patients were in glass rooms, no one was coming in and seeing them, and the care that was offered was modest, honestly, it was supportive care until patients need to go on the respirator, so to sit in the hospital on oxygen, terrified day by day by day, no one being able to come in the room, not being able to see their family, these messages got out to other family members and it put America on watch with extraordinary fear. Now, over the last year, I've published, and I've managed to get this out, despite our incredibly difficult publication cycles, I've published 40 peer-reviewed papers on COVID-19, that may be more than anybody in America. One of my very first papers, the title of it, and the paper dealt with what are the important outcomes? That's hospitalization and death, and when I started to see that scoreboard come up on the major media channels where it listed positive cases and death, and all the Americans remember this, this was up there almost instantaneously, it came from Johns Hopkins, instantaneously, it was cases and deaths, and I kinda wondered, how did they get that information so quickly?
0:11:43.7 DM: That was amazing. We don't have death certifications and other things that are very rapid at all, and who could be determining this, but in any way, it was up there, and what I said was, I said really what we need to know is who's being hospitalized, because if we can't figure out who's being hospitalized, and we can't figure out where the hospitalizations are occurring, we don't know where to allocate resources. So I published a paper on this in the journal that I edit Reviews in Cardiovascular Medicine, I immediately wanted to reach the American public, I published an op-ed in The Hill, which is a newsletter out of Washington, and I said, Listen, there's an emergent need, we need the hospitalizations. And I screamed as loud as I could to the administration to say, Listen, get an executive order to get the US hospital census every day so we could see what was going on. It never happened. We got an executive order to get the positive test results to come in from all the major laboratories and through the hospital laboratories because all the tests for the virus were under the emergency use authorization, so it was linked to an executive order.
0:12:54.6 DM: So the positive tests were just coming into the Johns Hopkins Center, so we knew who was test positive, there was no control over duplicates by the way, so if a patient had one or two or three tests, unless the system had a way of actually filtering out these duplicates, those piled on, and it really didn't take into consideration who was sick and who wasn't sick, so we just had test positive and then we had the deaths, which started to take on a cadence of trailing by about four weeks after the positive test cases, but that whole death ascertainment was a real mystery to Americans, and what I said, I think it was around March or April, I basically made the statement relatively publicly, I said, Listen, there are two bad outcomes, hospitalization and death. I'm gonna put together a team of doctors and figure out how to stop these hospitalizations and death. I felt compelled as an academic leader in medicine, if no one in the White House can say that... No one in the White House task force could say that, if no one in the FDA could say that, or the NIH or the CDC, and Americans were pouring into hospitals and dying, no one could make that courageous statement. Uniquely and individually and alone I made that statement.
0:14:20.9 DM: We had as our country's leadership, an inability to frame the problem. The problem was there was a virus, it was popping up in clusters in the United States, and in most people it was causing a cold and they got through it just fine, in other people, It was leading to hospitalization and death but we couldn't frame the problem that the virus in some people causes hospitalization and death, let's stop it. Let's stop the hospitalizations and death, let's treat the virus, we could not frame that problem, our leaders couldn't frame that problem. I personally didn't have any problem framing the problem. It's a bad thing. If there was another form of pneumonia out there, I would have said the same thing, another form of newly acquired asthma, another form of a urogenital infection or gastrointestinal infection. Ebola had just been actually in Dallas a few years earlier, and I think Ebola hurt us in terms of our thinking, because Ebola was so terribly contagious and so quickly fatal that the fear that Ebola created in Dallas was extraordinary. I'll never forget at our medical center one time I tried to get in one of the usual doors that I go into and there was a police officer there, I said, What's going on? He goes, We're here to block anybody with Ebola from coming in our hospital, we're going to shunt them to Presbyterian Hospital north of us.
0:15:55.7 DM: When do we shunt patients away from one hospital... The fear that Ebola created because of this idea was terribly contagious and fatal quickly, I think set us on edge, and with SARS-CoV-2 virus, what we learned is the average person sits at home for two weeks, there's no immediate lethality to the virus. In fact, we've got a long window of time to make a diagnosis, organize treatment, and prevent hospitalization and death. So SARS-CoV-2 was very different from Ebola, but we look at other conditions where we readily accept the fact that somebody can fall ill at home, but if we start treatment early with an infection, we can save the patient. That exists for community-acquired pneumonias. It occurs for various forms of staff infection, staphylococcal toxic shock syndrome, it occurs for diverticulitis and abdominal conditions, it occurs for skin infections, various forms of cellulitis. It occurs from meningitis. For instance, if someone had a forming meningitis, we wouldn't say, Listen to sit at home for two weeks, and then if you're really, really bad and you're having seizures and you can't even breathe anymore, then come in the hospital and we'll start treatment.
0:17:14.9 DM: So the different unique aspect of the medical response to SARS-CoV-2 and COVID-19 was for the first time we had an infectious disease where the medical community settled into a groupthink, and this was supported by the NIH, the CDC, the FDA, the American Medical Association, all the medical societies, it was supported by these societies to tell doctors, don't touch this virus, let patients stay at home, let them get as sick as humanly possible, and then when they can't breathe anymore, then go to the hospital. In fact, it was shocking in October 8th when the National Institutes of Health came out with our first set of treatment guidelines, because prior to that, none of the societies had any treatment guidelines, they actually didn't tell doctors how to treat the illness. Now there were suggestions about what should be done in the hospital but Americans cared about what was going on when they got sick at home, and the first set of guidelines said, you get sick at home, don't do anything. Don't do anything, come into the hospital when you really can't breathe, still don't do anything. Until a patient needs oxygen, then start doing something, then actually give the first anti-viral drug, which was Remdesivir.
0:18:32.0 DM: Well that's 14 days after the virus had already started replicating, by that time, the virus is long gone. When people can't breathe, the problem is micro-blood clotting in the lungs, so the federal agencies, CDC, the NIH and FDA, were enormously inept in terms of perceiving what this problem was. Incredibly inept in applying any type of judgment or direction to doctors. And what had happened among the doctors was we're so terribly frightened, we're not gonna do anything unless we have the intellectual support from our associations, from our federal agencies, from our medical societies, and it was just the opposite of what medicine had always been. Medicine had always been early innovation by doctors, empiric treatment, small studies, randomized trials, and then sponsored large randomized trials in that order, and then after large randomized trials, then guidelines bodies would then look at all those large randomized trials, make determinations of what should be done, and then those guidelines bodies would issue guidelines, and then the federal agencies would follow the guidelines. That's exactly what we do for mammography, colonoscopy, treatment of myocardial infarction, treatment of pneumonia. It always started out with early empiricism, then getting to guidelines and agency statements years later.
0:20:00.2 DM: It was a dangerous assumption to assume there's nothing that one can do for a fatal infection is enormous blunder, it's a blunder by citizens, it's a blunder by health responders, and it's a massive blunder by agencies. Can you imagine... Let's make an assumption, and could our assumption lead to the absolute worst possible outcome, which would be hospitalization and death?
0:20:29.0 DM: Or we can make another assumption and say, You know what, it's treatable, we're gonna try to treat it, which assumption is more dangerous? Absolutely, the dangerous assumption is to do nothing, the dangerous... You could take any example, let's make an assumption on traffic safety, you can assume that traffic safety rules and lines and stop signs and seat belts do something, or you can assume they don't. Let's try and let's have a free for all out on the streets right now and see what happens versus pay attention to some rules. We never make assumptions that are dangerous to people, and the thing that really worried me about this whole thing is this series of extraordinarily dangerous assumptions. Can you imagine a senior citizen who has heart and lung disease, recovered from cancer, has some kidney disease, is handed a diagnostic test result and says, Here you have COVID-19, now you have your fatal diagnosis. Our recommendations based on the assumption, we can't do anything, is go home and wait it out, and when that panic and that fear and that breathlessness and that fever is so overwhelming, when you can't bear it anymore, then go to the hospital and...
0:21:42.1 DM: How do people go to the hospital? They call family members. They contaminate all their family members. They call EMS, Uber drivers, taxi drivers. Every hospitalization in America was a super spreader event. So this assumption that there's nothing we could do, and giving somebody a fatal diagnosis with no instructions led to a massive amplification of cases. So what we could have assumed and what I did assume was that there are some principles we can adopt from other precedents. For example, every form of pneumonia known to man does better if treated early, even influenza. And that's the reason why Tamiflu, as an example, and there's an analogous product RFDA-approved for the treatment of influenza. They have some partial effect. Now, do we ever use Tamilflu alone? No, we typically combine it with other drugs to get patients through the illness. There are supportive respiratory drugs. There are forms of inhalers, what's called beta-agonist inhalers and steroid inhalers. We use those liberally in forms of emphysema, pneumonia, asthma, allergic pneumonitis. There's other things that we can do to help patients get through the syndrome.
0:23:00.1 DM: The inflammatory nature of the syndrome became very interesting. We understand that antihistamines, as an example, montelukast, aspirin, steroids, corticosteroids, play an important role. If I had an asthmatic at home, I wouldn't say, "Listen, sit at home for two weeks until you can't breathe anymore, and then go into the hospital." Are you kidding me? I'd put that asthmatic on inhalers. I probably would use some empiric antibiotics in that patient, and then some steroids, and I'd prevent the hospitalization to the best I could.
0:23:34.7 DM: So I approached COVID-19, respiratory illness, like any other, with the following thought, and we had pretty quickly put together our approach based on other precedents, including influenza, including asthma, including bacterial pneumonia as follows: That this was gonna be amenable to risk stratification. Those under age 50 who had no pulmonary symptoms, they could simply ride through the illness. We had data suggesting that nutritional deficiencies seemed to increase the risk for hospitalization and death. And so that's where the nutraceuticals came in early on, that there was supportive data, now, not curative, but supportive data for zinc, for vitamin D, vitamin C, and interestingly, a polyphenol substance called quercetin or querceten. There were some others that were considered, including lysine and N-acetyl cysteine. They became what we called the nutraceuticals bundle, so it was reasonable to do that. And patients would say, "Yeah, if it's linked to mortality, we don't know anything else. There's no harm in these supplements, they're readily available, people can buy them."
0:24:40.4 DM: So we recommended the nutraceuticals bundle for those under age 50, and really, no medical treatment. That amounted to, roughly, of people getting ill at the time, probably two-thirds to three-quarters of patients really needing no treatment. However, if someone below age 50 with medical problems presented with severe symptoms or over age 50 with medical problems, it became clear that the rates of hospitalization and death were greater than 1%. That was enough, greater than 1% is a magic number in this whole equation, that's enough to do something, that's enough to do something. We knew somebody at age 60, for instance, would face about an 18% chance of hospitalization and death, 18% chance, that's too high. In my field, cardiology, our guidelines say anything more than 5% is high-risk; 1%-5% is moderate, less than 1% is low-risk. In general, for anything less than 1%, we don't go after it. So in this low-risk group, we didn't go after it, but age over 50, young people presenting with severe symptoms, we went after it, so it was nutraceutical bundle.
0:25:44.1 DM: What did we know next? The timeline was very interesting. We knew from SARS-CoV-1, SARS-1, that's 80% similar to SARS-CoV-2. We knew from studies dating back to 2006 that hydroxychloroquine, a drug that's used for lupus, it's used for rheumatoid arthritis, it's used for other rheumatologic conditions, including dry eyes, as well as malaria, safe, was effective in reducing the viral replication of SARS-CoV-1, we knew that. And so United States knew that. In fact, that drug was stockpiled by the United States government, Australian government, some European governments. So hydroxychloroquine was onboarded appropriately and ready to rock and roll. In fact, many countries frontlined hydroxychloroquine for high-risk patients, and still do so today. We would go to Athens, Greece, Rome, Italy, across all of Eastern Europe, Central and South America, hydroxychloroquine is the lead drug. India and East Asia, hydroxychloroquine is the lead drug. So hydroxychloroquine played a role. We also knew that by the summer, we knew that ivermectin played a role. This is an anti-parasitic drug used for scabies and other illnesses, safe and effective.
0:26:56.3 DM: So these drugs, the reason why they work against the virus is they get inside cells. A lot of the antibiotics like penicillin doesn't get inside the cell. But these what's called intracellular anti-infectives do. Japan had an influenza drug that had the exact same activity as remdesivir, their first US-approved inpatient IV drug. That drug's called favipiravir, and the Japanese had data to suggest that favipiravir, like oral remdesivir, would play a role early on, and it was readily approved by five countries, FDA-approved, FDA-equivalent approved in those countries to treat COVID-19.
0:27:33.0 DM: So we had hydroxychloroquine, we had ivermectin, favipiravir. We combine it with either doxycycline or azithromycin, those are antibiotics Americans know about. They get inside of cells. They're also intracellular anti-infectives, and and they were slightly assistive in a couple ways. They cut down on some of the bacterial superinfection that would occur in the sinuses and respiratory tract. And we knew for some studies that there was about a 3% overlap between COVID-19 and what's called atypical pneumonias, which would be mycoplasma chlamydia pneumonia, and these would also be responsive to these. So quickly, hydroxy and azithro, ivermectin and doxy, these were a common... Favipiravir and doxy outside the United States became common intracellular anti-infectives.
0:28:16.5 DM: But those alone didn't carry the day because what happened is the viral replication tipped off what's called cytokine storm, or the immune system going haywire. And so doctors, early on, in the hospital started using steroids. And we had some confusing literature, "Are they hurting? Are they helping?" And the British helped out a lot with a study, an inpatient study called the recovery trial. And the recovery trial picked an odd corticosteroid, which is dexamethasone, in an odd dose, 6 mg a day. We typically use 10 mg four times a day. So an odd dose, but did show a small reduction in mortality. And there was a meta-analysis published looking at hydrocortisone, prednisone. It turned out any steroid worked in some reasonable dose. So in the United States, we quickly adopt using prednisone, which we use in asthma, frequently.
0:29:06.0 DM: And then another trial in the UK was done called the stoic trial using inhaled budesonide. Now, that was a very interesting development because there was a maverick doctor, former military doctor, Richard Bartlett from West Texas. He would make the national news by saying, "You know what? I think inhaled budesonide works." And he said this early in the spring, and he was on national news, he said, "You know, I'm trying it. I'm a doctor, I'm trying to help my patients. I am using empiric treatment. I know there's no randomized trials," but he was doing the right thing. That's what American doctors all should have been doing, is trying to help their patients by taking empiric choices on drugs that made clinical sense, and he tried it. And indeed, it worked. The British did the stoic trial, and sure enough, there was over an 80% reduction in hospitalization if we just used inhaled budesonide in outpatients with COVID-19. So that made it onboard.
0:30:00.6 DM: Montreal Heart Institute, one of the leading overall randomized controlled trial centers in the world got funding from the National Institutes of Health, Gates Foundation, Canadian authorities, and tested a gout drug, which works against the immune system, particularly works against the white blood cells and their ability to proliferate toxic granules and assemble microtubules, that drug is called colchicine. So Americans will recognize this as a gout drug. They carried out and conducted a prospective randomized trial, double blind for 30 days, the best quality trial done in all of COVID-19, and they demonstrated that there was a marked reduction in hospitalization and death. So colchicine came onboard.
0:30:46.0 DM: And so the last thing that we really had to look at was blood clotting. And to this day, there has not been a single outpatient study of drugs to impair platelet aggregation or antithrombotics. However, we can learn from inpatient studies, and there's been very good analysis, they all agree, the use of full-dose aspirin in the hospital is associated with reductions in mortality, and the use of full-dose anticoagulation, whether that be injectable, low-molecular heparin, full heparinization, or we can even use oral anticoagulants as an outpatient, is associated with reductions in mortality.
0:31:22.2 DM: So what I had been doing is I was working with the Italians looking at how these concepts are coming together, and I published a paper in the American Journal of Medicine in August of 2020. And I have to tell you, when I looked at the literature through the spring, working with the Italians, there had been... When at the time I submitted the paper on July first, there were 55,000 papers in the peer-reviewed literature. Not a single one taught doctors how to put drugs in combination and treat the virus. And it seems so odd to me. We knew this was a fatal viral infection. In fatal viral inflections, single drugs never work. We knew this in HIV, we knew that we needed multiple drugs in HIV. We knew this for Hepatitis C. We knew this for all the other fatal viral infections. We use drug combinations, never single drugs. And the only thing we could do at that time is look at studies of single drugs and find signals of benefit, acceptable safety, and then assemble them into regimens. The clinical trials testing a four-to-six-drug regimen, those haven't even been planned yet.
He published The Pathophysiologic Rationale ,,,
0:32:31.7 DM: The mortality rate would have been astronomical if somebody didn't step forward and have the courage to publish the concepts. And I guess that's what my role is in world's history for this. I pushed a paper called The Pathophysiologic Rationale for Early Ambulatory Treatment of COVID-19, and it was published in the August issue of 2020 of American Journal of Medicine. To this day, that's the most widely downloaded paper from that journal of all topics. And it went viral. And literally, it went viral because the world was thirsting for an approach to COVID-19.
0:33:11.1 DM: Now, quickly after that was published, I was managing all different types of communications regarding the paper, scientific and then also media-related. And we had supportive data now coming in strong for ivermectin, for colchicine, for inhaled steroid. And Operation Warp Speed had delivered monoclonal antibodies directed against the spike protein, the pathogenic part of the virus, and they included a product from Lilly and another one from Regeneron. So I needed to update the algorithm, and I put that together and published that in the journal that I edit Reviews in Cardiovascular Medicine, but with a separate issue and a separate, unbiased editor that I didn't have influence on to make sure that was fully peer-reviewed and vetted, and which it was. And that was published in Reviews in Cardiovascular Medicine in August of 2020.
0:34:00.6 DM: By that time, there was 100,000 papers in the literature. And outside of my first paper, there wasn't a single other paper that actually proposed a regimen or a protocol to treat patients with COVID-19. It was almost extraordinary that we were over nine months into a fatal pandemic influencing the world, and no one could come up with an original idea of how to put drugs in combination to treat the virus? We didn't have the Harvard protocol, we didn't have the Johns Hopkins protocol. We didn't have UCLA, we didn't have a World Health protocol. So this was extraordinary that all the firepower we had in academic medicine couldn't... They just drew a blank. Matter of fact, if you look at these centers across the United States and across the world, they never opened up COVID treatment centers. They didn't have outpatient COVID treatment centers. They didn't attempt to study or help a single outpatient with COVID-19.
0:35:06.0 DM: My contribution was, I think, the ability to publish the ideas.
0:35:11.8 Speaker 2: Okay.
0:35:12.0 DM: This is very important. Others had the ideas. Vladimir Zelenko in New York City, Orthodox Jew, stepped out of the box. He said, "Listen, we need to treat this. We can use some drugs in combination: Hydroxychloroquine, azithromycin, steroids, other drugs." And he started putting drugs into combination. Richard Bartlett in West Texas. Brian Tyson and George Fareed, former NIH scientist, George Fareed came out of retirement. They went to, really, the crucible of COVID-19 down in the California-Mexico border, and just opened up a clinic and had opened up a tent. People started walking up and they started treating them. Didier Raoult in Southern France said, "Listen, we can treat this." Him and a group of courageous French doctors opened up a large clinic in Southern France and started treating patients. We had Ivette Lozano in Dallas. She took her general practice building by White Rock Lake and turned it into a COVID treatment center. She converted all her rooms to treating patients with COVID, oxygen concentrators, had all the drugs. There's pictures of patients lining up on the sidewalk to receive treatment.
0:36:22.8 DM: So it was interesting how the innovators were all independent, courageous doctors; and the academic medical centers drew a blank. They couldn't even pitch a tent to help people. And to me, it was stunning that the academic medical centers or even the large community centers couldn't help a single outpatient. They couldn't even provide a patient brochure of what should be done. The CDC offered guidance like, "Take some Tylenol. And if you get really sick, go to the hospital." The response to a treatable outpatient problem, they gave us two weeks of opportunity to do something. The lack of that response was stunning. And it had to do, in my view, because of a whole timeline of events that put a chill on the attempts to treat COVID-19. Doctors in health systems and others, I think, in a relatively short order, became actively discouraged from treating COVID-19.
No positive feedback from his paper
0:37:23.5 DM: I can tell you I never got an encouraging email or phone call saying, "You know what? Do the best you can for your patients. Try to help them. These hospitalizations are terrible. Please, we support you in using your best judgment." Or, "Here's a few suggested things that you could do." I never got any of those emails from medical societies, from others. In fact, there was only one medical organization; just like there's a few courageous medical doctors, there was one courageous medical organization, the Association of American Physicians and Surgeons, that saw what was going on. And interestingly, that organization is an organization that represents independent doctors; not those employed by hospitals or big medical groups or medical schools, but independent doctors. And they saw what was going on, and the first thing that they attacked was the stockpile of hydroxychloroquine.
0:38:12.4 DM: So what happened was the US had an ample supply of hydroxychloroquine, and the only issue was, "Start using it and start putting it into combination with other drugs to treat COVID-19. It seemed terrific." And the first event in the timeline was the FDA emergency use authorization for hydroxychloroquine. So the listener should understand that an emergency use authorization would be for a brand new drug or product where there is a great unmet need, there's not enough time to do all the testing, and that we would do an EUA for that. There's a government mechanism for that, and it's under emergency circumstances. That wouldn't apply the hydroxychloroquine. It was already fully FDA-approved, it was out for 65 years, it was safe. We had used it in pregnancy. We knew all of its safety profile. Doctors knew how to use hydroxychloroquine. I use it in my practice. It was just not a big deal, it didn't need an EUA.
Emergency Use Authorization for hydroxychloroquine
0:39:06.2 DM: But so the EUA went out on hydroxychloroquine and said, "You know, this EUA," with language, and it says, "Restricting hydroxychloroquine to inpatient use." Okay. And so one of the first big studies out of the block was done in thousands of patients out of Henry Ford. And it was great news that hydroxychloroquine was associated with a large reduction in mortality if applied early. But the later it was applied in the hospital stay, it didn't look like... Patients were too far gone. I wrote the response to that in several publications across the United States, and one was an op-ed in The Hill. 'Cause as I saw this, I basically made the case that that emergency use authorization was an effective restriction. It should be lifted and we should use hydroxychloroquine wide open.
0:40:01.7 DM: And then something really terrible happened. Keep in mind that the Henry Ford data was very positive. We had the EUA, the US had stockpiled it. The National Institutes of Health, the Allergy and Immunology Branch had commissioned a several thousand prospect of double-blind randomized placebo controlled trial of hydroxychloroquine and azithromycin in outpatients with COVID-19. They had funded the trial. They got the drug supply. They got the placebos. They set up all the study centers in the United States, we were all ready to go, that was in the spring. Terrific! Everything's coming together. And then what happened was a fake paper was published in Lancet. A fake paper.
Fake paper published in Lancet
0:40:46.9 DM: Now, Lancet, the listener should understand that Lancet is like the New England Journal of Medicine. It's one of the most prestigious medical journals in the world. When a paper is submitted, there are so many checks on validity. Where is the paper coming from? Where are the data coming from? Validating the data. Then it's sent out to peer reviewers who are independent. They check everything in the paper. They give comments about, "Was this reported? Was that reported?" What have you. There's so many checks on papers. And then it comes back, and then there's an editorial decision made on a paper, and then it's published. That's called peer review. That ensures to the public that papers are not fake. It's very important. And it ensures to the public that things are not falsified.
0:41:31.7 DM: Well, this paper had authors from Harvard. It came from a company called Surgisphere that no one really understood what this company was about. And the data was a large data set of inpatients with COVID-19 from all over the world that had in-depth drug exposure data. We didn't have that back then. That was from December, January, February. This was just emergent. We didn't have this. The average age in that paper was 49 years old. And the paper implied that use of hydroxychloroquine was dangerous. And Lancet published this falsified paper. Somehow, it fell through all the other peer review... And how could they possibly publish it? And as soon as it came out, I knew in two seconds that it had to be wrong. We don't hospitalize people in their 40s. And hydroxychloroquine, in fact, is associated with benefit, not harm.
0:42:24.1 DM: This paper in Lancet frightened the entire world. It was like a shockwave. And there was a whole series of reactions. People started publishing papers, "Oh, hydroxychloroquine could be dangerous. All these academic doctors, case closed. Hydroxychloroquine doesn't work, stop using it." Hospitals started pulling it off their formularies. It was extraordinary what happened with hydroxychloroquine. In fact, the US FDA put out language that said, "Hydroxychloroquine shouldn't be used, period. We're cancelling the EUA for inpatient use, and it shouldn't be used, period." So that FDA language then went to the AMA. And the AMA says, "Well, don't use hydroxychloroquine, period, inpatient or outpatient." That went to the pharmacy boards. Pharmacy boards said, "Oh, doctors shouldn't be using this."
0:43:08.3 DM: So as doctors were treating patients in the community, prescribing hydroxychloroquine, the next thing you know, patients would show up to the pharmacy and the pharmacist said, "Sorry, I can't dispense it. My board says that I can't," and then doctors' licenses started to become threatened, and then all of a sudden there was a cascade of events, hydroxychloroquine being the lead that put a chilling effect on anybody's attempt to treat COVID-19 as an outpatient.
Hydroxychloroquine - the most studied and used therapeutic
0:43:41.3 DM: Hydroxychloroquine, I think the fair statements are, it's the most studied and utilized therapeutic in the world for COVID-19 today. There are hundreds and hundreds of studies. And hydroxychloroquine was appropriately acquired and stockpiled by the US Government. President Trump, who I personally think was very weak in the response, he could not articulate that hospitalizations and deaths were a serious problem. He could not assemble a team of doctors who were learning how to treat COVID-19, neither could the NIH or the CDC or FDA. We had gross failures from US Presidents and the major agencies. Can you imagine to this day, we still have not had a doctor in any position of authority in the United States who's actually ever seen a patient with COVID-19 and treated them? None. It is extraordinary what's happened. So, President Trump mentioned hydroxychloroquine, let's try to give it a shot. And then immediately he was bashed down by his detractors. I thought it was a very weak statement to begin with, but he was bashed down and people have always held him up as, "Oh, it was Trump. If he hadn't mentioned hydroxychloroquine none of this would have happened."
Enormous effort to suppress early treatment. Hydroxychloroquine
0:44:51.3 DM: I disagree. I think that there was an enormous effort to suppress early treatment. Hydroxychloroquine was the initial lightning rod. Remember I mentioned that NIH trial? You know what they did after 20 patients, disingenuously, they said they couldn't find COVID-19 patients, and they shut down a several thousand patient trail. They shut it down after 20 patients. That never happens. They purchased the placebo, they found the study centers, they had the binders, they had the nurses hired, they had everybody ready to treat Americans with hydroxychloroquine and azithromycin and they gave up after 20 patients. That was extraordinary. The false paper published in Lancet was extraordinary. We started to have an array of incredibly flawed papers publishing exaggerating cardiac effects of hydroxychloroquine. Oh, it could cause dangerous arrhythmias.
Hydroxychloroquin not cause scarring of the heart
0:45:43.8 DM: There was one that I mentioned in my US Senate testimony came from the Mayo Clinic, it said hydroxychloroquine can cause a scar in the heart, they actually... They had a heart and they showed a huge white scar. In fact, I ultimately hunted down that paper, hunted down the authors and the publisher, and I demanded a retraction, and ultimately I got a conciliatory letter published saying, you know what, we're sorry, it doesn't really cause a scar in the heart. So people started to intentionally try to damage hydroxychloroquine so it would not be used in COVID-19. Yet other countries held with it steadfast. I mentioned all the countries to this day that use hydroxychloroquine, and now we have studies, for instance, a study from Iran in 30,000 patients, a massive study, and they treated about 25% of people appropriately, hydroxychloroquine in combination with other drugs, and it has a massive reduction in mortality.
Hydroxychloroquin is useful, but not as a single drug
0:46:35.7 DM: So, hydroxychloroquine is a mainstay, the prospective randomized trials, we just isolate on them, pre-hospital studies are all positive. Now, is it a game changer? No, I'd say it's about a 25% reduction in endpoints, but it's a very useful drug to get started early. It's not a single drug, I wouldn't rely on it alone, but hydroxychloroquine itself I think is a poster child for what happened. You know, early on in this I became of national attention, I received calls from the White House. I was contacted by the US Senate. I became known on social media, which I was never on social media before, I'm not an immunologist, I'm not a virologist, I'm not an infectious disease doctor, but I'm a good clinical doctor, and I understand drugs, and I understand drug safety very well. Hydroxychloroquine had a single benefit, acceptable safety. I was contacted by doctors in Africa that anonymously told me, Dr. McCullough, there are some bad guys raiding the pharmacies at night, and they're coming in and burning the hydroxychloroquine.
ivermectin and FLCCC
0:47:41.3 DM: I said, Who are these bad guys? They say, We don't know, but they look like there's some type of mercenaries or operatives. Mysteriously, the second largest hydroxychloroquine producing plant outside of Taipei burned to the ground. So, hydroxychloroquine as a simple, safe, and effective drug to this day seems to be a poster child for worldwide comprehensive efforts to suppress early treatment. And of interest, as the data came out with ivermectin, ivermectin became the next drug. Now, of interest with ivermectin, there was an associated group that formed called the Front Line Critical Care Consortium, FLCCC, it was led by Pierre Kory. I identified him and Dr. Paul Merrick, I communicated with him. We had teleconferences and I recommended Dr. Kory testify at the second US Senate hearings in December. Also, Dr. JJ Rajter from Florida.
0:48:42.9 DM: Dr. Rajter had tried hydroxy... Had tried ivermectin in all of his sick patients in Florida hospitals and was enormously successful in reducing mortality. Published his paper in Chest one of the best pulmonary journals, so I gave him tremendous credit for that. And so, Dr. Kory and Dr. Rajter presented what became a very compelling case for ivermectin. If people were sufficiently turned off by hydroxychloroquine, we could focus on ivermectin. Dr. Tess Lawrie, who is considered one of the world's most prominent analysts in the UK, published, and Dr. Andrew Hill as well, published incredible analyses demonstrating that ivermectin reduced mortality in-patient and out-patient. So a little different than hydroxychloroquine. Hydroxychloroquine takes a little time to work and probably doesn't work at the very end of the illness, but ivermectin miraculously work through the range of illness.
hydroxychloroquine and Ivermetic used for prevention and early treatment
0:49:37.6 DM: And so, the data started coming on for ivermectin and there was enough push power for emphasis on the National Institutes of Health guidelines where they made a specific statement regarding ivermectin. They said, You know what, we understand the data with ivermectin, we can't be for it, and we can't be against it. It's the same statement that they made for the emergency use of Regeneron and Lily antibodies. If the... NIH, we understand the data, we can't be for it or against it. But at least we got a neutral statement out of them. Hydroxychloroquine still to this day has a series of negative statements on this, and doctors have literally had to fight for their medical licenses in order to prescribe hydroxychloroquine. One by one by one, all of those licenses have been restored, all of those state rulings have been overturned, all the medical societies has been overturned and hydroxychloroquine is used today. Ivermectin is widely used today. Both drugs can not only treat the infection early, but they can prevent the... There's prophylactic studies, they can prevent, if patients take these drugs periodically, typically once a week or so, they can prevent COVID-19 from becoming an illness, they are preventive.
0:50:45.9 DM: In fact, I led one of the very early studies of hydroxychloroquine here in Dallas to protect our healthcare workers. That these drugs are about 90% effective, they are about as effective as the vaccines in preventing acquiring COVID-19. When someone's ill, I never prescribe these drugs alone, but I prescribe them in what I call sequence multi-drug therapy. But that is the approach that independent doctors have taken in the United States and uniquely, not a single academic medical center today or a community medical center today treats COVID-19 patients as an outpatient with the goal of reducing hospitalizations and deaths. Why would these centers not wanna help their patients?
Drs. unable to get consensus when they could not meet during COVID-19
0:51:45.2 DM: You know, doctors clearly have a groupthink, and doctors want intellectual support for what they do. That's the reason why we meet all the time, that's the reason we go on rounds together, that's the reason why we have conferences every day, we want to intellectually support each other for making decisions on patients for the assurances we're making the right decisions. And what happened was with the pandemic, all of our meetings were dissolved, we could not meet with each other anymore, there wasn't a chance to have much intellectual support, and each doctor one by one had to make a decision. When the next patient called and said, "Listen, I'm sick with COVID-19, can you help me?" There was a binary choice, the choice was, No, "I'm not gonna help you, nothing works, there's nothing I can do, just wait until you get hospitalized," or the answer could be, "You know what, let me try."
His father got COVID-19 and was treated by zinc, vitamin C, vitamin D, quercetin, etc.
0:52:37.9 DM: And what we found is that binary choice was the biopsy of who really had courage and who really had excellent clinical judgement. And doctors who are not confident in their clinical judgment quickly said, You know what, there's nothing you can do, and they got into that groupthink and that could have been 90% plus of doctors had A, a lack of clinical judgment and a lack of courage. And what I found in this whole thing is, those two things are rare. And for me, it was just very natural. It was very natural. My father was one of the first nursing home COVID-19 patients in Dallas, he was the very first one at Presbyterian Village. He got COVID-19, he had pelvic fracture, he's flat on his back, then a scared PA says, Your dad's got COVID, he's in a unit. We don't know what's gonna happen. His mortality, being completely bedridden with dementia, and now COVID, I can tell you, he was facing an 80% mortality of just having COVID just ravage him.
0:53:44.1 DM: So what did I do? Did I make that binary decision of doing nothing? Of course not, of course not. If I could ever message any American doctor or any doctor in the world right now, have some courage and trust your clinical judgment. I did, and that's what real doctors do, and I will never apologize for that. Of course, my dad was treated with hydroxychloroquine, he was treated with azithromycin, he was treated with aspirin. We put him on Lovenox, it's a blood thinner. The full nutraceutical bundle, zinc, vitamin C, vitamin D, quercetin, open the windows, get that virus aired out there. And he got really sick, as expected. He had dementia, his wishes were to not go to the hospital, not go on a mechanical ventilator, we treated him right there. It took 60 days and it was a long illness, but he survived.
0:54:42.4 S2: Impressive.
0:54:43.2 DM: And that was early. And that taught me that if I'm willing to do that for my father, I have a Hippocratic Oath, and I have a fiduciary responsibility to my patients. And I refuse to let my patients die of this illness. And when I testified in the US Senate, I told the American people, I have always treated my high-risk patients, always. And at the end of my opening statement, I held up the protocol and I told the American people, I'm not asking for permission to do this, I'm not, but I'm asking for your help. That's a very, very important statement, because my patients were appropriately treated to the best of my ability, and we have 600,000 dead Americans that were not treated appropriately and not treated to the best of the ability of their doctors, and that will go down in historical shame for our country. I think it's a travesty that we have 600,000 dead Americans, vast majority of them didn't get an ounce of treatment.
our methods could reduce hospitalization and death by 85% - We're treating 10,000 to 15,000 patients a day.
0:56:00.4 DM: In fact, there were medical groups that adopted policies that they weren't gonna even answer the calls of COVID-19 patients, and there were millions of patients needlessly hospitalized. We had data that came in later from Dr. Zelenko, New York City, Dr. Proctor here in Dallas, who did the same exact thing, showing that our methods could reduce hospitalization and death by 85%. And I'm sorry, there are no prospective randomized trials of four to six drugs, there are none planned, so therefore, without any large trials, there were not gonna be any guideline statements, and without any guideline statements we'll never have any agency support for this. But this is about courageous doctors saving Americans, and I would go farther than this, this is about courageous doctor saving the world. So now we have the Association of American Physicians and Surgeons, we have FLCC in the United States, we have 250 treating doctors, we have four national telemedicine services, 15 regional telemedicine services. We're treating 10 to 15,000 patients a day.
0:56:57.2 DM: Forget the US Government, forget what anybody says about this, Americans are getting treatment, that once our message on early treatment came with two US Senate hearings headed by Senator Ron Johnson, the hospital started clearing out in the end of December, early January, because early treatment markedly reduces spread and dramatically reduces hospitalization and death. It's the only thing that does that. The hospital doesn't save all the patients. I'd say the hospital honestly has a very modest impact on anything with COVID-19, it's all about early treatment. The hospital started clearing out, the curves came way down in the United States, that's before anybody was fully vaccinated. And I testified in the Texas Senate on March 10th, I said listen, by standard CDC equations, we're at herd immunity. By March 10th, no vaccine effect. That's actually just treating patients.
South Africa success customizing treatment to each patient
0:57:46.2 DM: In Texas, we had 35 treatment centers, our protocols and methods work, and I have learned over time, there are so many ways to treat the virus. I've had a seminar with Dr. Shankara Chetty in South Africa. He said that hydroxychloroquine and ivermectin, just like in the United States have become so politically charged, doctors were losing their licenses, in fact, some doctors were jailed in trying to help patients with COVID-19. He gave up on them. He's treated 4000 patients. Fewer than 10% got hydroxychloroquine or ivermectin. He treats them, he times the illness, he waits to day eight and then he starts inhaled on oral steroids, he starts aspirin, other anti-inflammatories, montelukast, and the hybrids patients who uses anticoagulants on the backend, and he saved virtually everyone outside of a handful of patients out of 4000, sick patients in South Africa.
0:58:34.1 DM: So what I've learned about this virus is if doctors do anything to try to help patients, they can reduce hospitalizations and death, and the only reason why this is such a horrible thing in American history is because doctors failed to act.
40% of drug use is "off label"
0:58:56.1 DM: The US FDA puts out thousands of drug warnings per year. In fact, Americans know this, 'cause they see a drug advertised on TV and it says warnings, may cause death, may cause whatever, so we get thousands of warnings per year. FDA recalls drugs, put black box warnings on drugs, doctors still use these drugs, they understand the warnings. About 40% of drugs are used off the advertising label, so once a drug is older, its original advertising label doesn't really apply, so we use drugs "off-label" all the time, that's common. But what happened in COVID-19 is because of the tremendous fear that settled in over our country, whatever statements came up by the US FDA, the NIH and the CDC, started to take more weight than they ever would in the past. So, if those agencies said something like, Don't use hydroxychloroquine, that emanated down through the AMA and each of the pharmacy boards where they actually denied patients hydroxychloroquine. In fact, there are probably patients who died because the pharmacy did not dispense the hydroxychloroquine to patients, and/or the ivermectin.
1:00:05.4 DM: There are doctors who started getting warning letters, stating Dr. Richard Urso from Houston, another doctor stepped out of his role like I did to treat the virus, got warning letters from the Texas Medical Board, we're gonna examine your license, we understand you're prescribing hydroxychloroquine, trying to help COVID patients. Okay. These doctors, Dr. Robin Armstrong. Dr. Robin Armstrong in Texas saved dozens of nursing home patients with hydroxychloroquine, azithromycin, steroids, and blood thinners. The families think he's a hero, the Texas Medical Board tried to take away his license. And so, he had to go through hearings and reviews, and ultimately he was restored, although his practice was just damaged, if not destroyed. Email started coming down through big medical organizations, don't use hydroxychloroquine. They later on came down said, don't use ivermectin.
Drs being told to not treat COVID-19 with drugs
1:00:55.2 DM: In fact, there was... You know, flat out, don't do it. We were getting official messages that basically said, Don't take care of COVID-19. These are codified in policies and emails by major medical organizations, and it went counter... Can you imagine getting an email saying, Don't treat pneumococcal pneumonia, just let him die, don't treat meningitis, let him die? Can you ever... We've never seen this... This is the term that applies to what's going on is wrong doing by those in positions of authority, it's called malfeasance. We don't put down a chilling negative message that's gonna result in harm. We don't do that, we don't do that in a civil society, it happened from the NIH, the CDC, the FDA, major medical groups, these chilling messages. But at the same time, you had AAPS saying, No, this is wrong, treat patients. You had FLCC, a group that became very strong saying, No, treat patients. In the UK, we had the Bird Group, that said, You know what? Treat patients, use ivermectin-based protocols.
1:02:00.6 DM: We had PANDA develop in South Africa, we had the COVID medical network develop in Australia. We had treatment domiciliary develop in Italy. So listen, the counter-argument to this of no, we should treat the virus, that counterweight was there. And it's one of the reasons why you're talking to me today. You're not talking to some FDA official who basically wanted to throw cold water on things, you're talking to me today, because you're getting a sense of truth, you're getting a sense of reality that this virus is treatable. Everything that we've done for this virus, we've made it far worse by not treating it, keeping patients in fear, isolation. We've done multiple things that have promoted hospitalization, and we've done multiple things that have actually promoted excess mortality, and it's a shameful time in America and in the world.
FDA, etc say what not to do, but does not say what to do
1:03:00.5 DM: Under the dark cloud of fear, the medical administrations defer to the FDA, the NIH and the CDC, our three governmental agencies, they defer to that. In fact, they will state, we're following the policy. So let's pick something less charged, like wearing masks. What sets the mask wearing policy? What the CDC says, Well, they say this, let's follow it. Same thing is true, if the agencies say, Don't use hydroxychloroquine or ivermectin, if that's what they say, that quickly gets down to medical administration and they'll float out an email saying, Don't do it. In fact, in a country, we can pick on at Australia, they have the TGA, that's the equivalent of the FDA, they have guidelines where they literally have dozens and dozens of negative statements, don't do this, don't do that, don't do this, don't do that.
1:03:55.0 DM: Interestingly, none of these groups actually say what to do. So if you're to take any major hospital and ask them what email or what policy came down that tell doctors what to do? You gave warnings on what not to do, but what did you tell them to do, to take care of clinic patients with COVID-19? Most of them would say, Nothing. We don't have... In fact, I testified in the Texas Senate on this topic, and within March 10th and within 48 hours there was draft legislation, to at least give patients some information. So listen, if the hospitals and doctors aren't gonna do anything, we're gonna give you some information. Here is some... When you get your positive test result, here is some information on what you can do, here are the treatment protocols, here are the EUA monoclonal antibodies. And again, if hydroxychloroquine or ivermectin is controversial.
monoclonal antibodies - emergency use authorized, big money, but no updated information
1:04:46.1 DM: Okay, but what about the monoclonal antibodies? We haven't talked about these. These are high-tech, they're produced by big pharma, it's big money. It was all NIH-funded. They're emergency use authorized by the US FDA. How come America has no window to that? How come there's no updates on how we're doing with that? How come there's no 1-800 numbers, how sick patients can't find out where these antibodies are? So it is a global suppression of early treatment, whether they're generic drugs or newly-approved drugs. There is a global suppression on early treatment.
1:05:19.6 DM: Americans will know, they watch the TV every night. The initial dialogue was, "We're scared. Wear a masks, go on lockdown, hand sanitizer. Okay." Then there were some reports about terrible things going in the hospital. Then the reports later on were, "Wait for a vaccine." There were never regular reports or updates from any local or national TV source that gave regular updates. "This is what you should do when you get COVID-19 at home. Here are the drugs that work. Here are the protocols. Here are the hotlines, so you can get an antibody infusion, which is approved by the FDA. Here are the hotlines so you can get in research." Research is important. There's still no hotline for Americans to get in COVID-19 research at a state or a Federal level. Stunning! There's been no updates.
1:06:10.8 DM: When I've dealt with multiple congressional and senate offices, I say, "Listen, weekly updates to the American people so they know what to do, so they're not so in fear when they're getting these results. Weekly updates through all public channels. Weekly updates on treatment, and then monthly updates to the guidelines." We have none of that. We are over a year of this and the Americans have been absolutely let down by the government agencies, by the media. The media, why wouldn't it come in to any local broadcaster's thought process to give their listeners an update on early treatment? It's a stunning oblivion.
[pause]
1:07:04.7 DM: For products to actually be officially advertised, they have to have somebody who's gonna pay for the ad, which is a drug company, and they have to be FDA-approved, and they actually have to have an FDA advertising label. And because of the monoclonal antibodies, as an example, don't have an advertising label, they can't be... Lilly and Regeneron can't go out and advertise for them. But because they're EUA from a public health messaging perspective, they should be equally featured as vaccines.
Extensive "advertising" for vaccines, but nothing else
1:07:37.9 DM: Now, vaccines are emergency use authorized. All we hear about is vaccines morning, noon and night. Why do we hear a massive messaging about vaccines? Americans ought to think about this. Why are vaccines featured by the CDC, NIH and FDA morning, noon and night; by the media, morning, noon and night; by every medical center, morning, noon and night. I can tell you as a doctor in a medical center, all our emails are about vaccination. Why are they featured in every single public health communication, needles and all the arms? In fact, shockingly, in a Dallas area in October, this is long before the vaccine trials were ever completed, if you were to call CVS or Walgreens, the answering machine would say, "We're proud to offer the COVID-19 vaccine when it comes available." We have never advertised for a product before it comes available. In fact, it's against US laws regarding drugs and biological products.
1:08:40.9 DM: So things started to go off the rails very early on, and it seems like there was a playbook. The playbook was to suppress any hope of treatment, a complete oblivion to treatment through all the entities that we've mentioned, and at the same time, prepare the population for mass vaccination. These two are very tightly linked. And now with mass vaccination, we have... We see things we have never seen. Advertising the vaccine before it's even available. Massive messaging for the vaccine far out of proportion to treatment.
monoclonal antibodies being squashed, vaccines promoted
1:09:20.4 DM: You have two EUA products, one you never hear about. Americans are starved of these monoclonal antibodies. In fact, they're grossly underused. They could have saved probably tens of thousands, if not hundreds of thousands of lives, and they're being squashed. The Lilly and Regeneron products are being squashed. But the Pfizer, Moderna and J&J products are being massively promoted and advertised. Americans ought to be wondering, "Why is that happening? Why are we defocusing on the sick patient and focusing on well people? All the messaging about contagion control and vaccines are about well people. Why can we not focus on the sick COVID patient?" That was my message to the Department of Health and Human Services in Texas. But it goes further than that. It goes further than that.
Vaccines were not tested on pregnant women, but they are vaccinated anyway
1:10:08.8 DM: The vaccine registrational trials strictly excluded pregnant women, women of child-bearing potential, COVID-recovered patients, patients who had prior COVID antibodies; strictly excluded them. By regulatory science, if all the registrational trials excluded a group of patients, we would never use that product in that group once it gets on the market, never. Never, we never violate that. Why? 'Cause we don't know if it's gonna work, and we don't know if it's gonna be safe. We never do that.
1:10:40.0 DM: There's another level. With pregnant women are a special group in research and medicinal products. Very important for Americans to know this. In pregnant women, for vaccination, we only vaccinate with safe, inactive products; inactive flu, tetanus, diptheria and pertussis. That's it. We would never inject a biologically-active substance in a pregnant woman's body, that could be dangerous. Never! And with the vaccines, as soon as they came out, the CDC, FDA, media, everybody said, "Vaccinate them. Vaccinate them."
[pause]
Previous vaccines had 48 months of testing, this one had 2 months before getting EUA
1:11:29.3 DM: Well, the US FDA regulatory guidance and vaccines, and there have been modern vaccines, you don't have to pick the old ones. We've had modern vaccines. Shingles vaccines, hepatitis B, meningococcal vaccines demand a minimum of two years of safety data, two years, by regulatory. In fact, these are kinda written and codified into the regulatory rules for the manufacturers. That was all thrown out and said, "Two months. For COVID, two months." So two months of observational data.
1:12:03.3 S2: This idea that we could vaccinate people that were not even tested in the trials, that has never been done before. We have never just thrown a vaccine at somebody without having any data. None. So the very first pregnant woman that was vaccinated here in the United States, it was done with no knowledge of safety and no knowledge of efficacy. And the argument that we've heard is, "Well, COVID-19 is a bad illness; 600,000 people have died. The vaccine could help them, we should give it a shot. Come on, we should just give it a shot." Well, that 600,000 died, I've already told you, 85% of that was preventable with early treatment, which was actively suppressed and squashed. And not only that, is if this vaccine can help them, the vaccine better be safe. It better be safe. And my comments on the vaccine are, "Safety, safety safety, let's see it, let's see it."
1:13:03.9 DM: And Americans ought, just like the Americans should have been getting weekly updates on treatment innovations, Americans should have been getting weekly updates on vaccine safety. Very important. Weekly updates from our Federal officials on safety. Super important. Those two things are probably the two largest acts of malfeasance in all of medical regulatory history. It will go down in the history of malfeasance, wrongdoing by those of authority. How come there was no updates on treatment and no promotion of early treatment to reduce hospitalization and death? And now, when we release the vaccine, why are there no safety updates? Why are there no attempts for risk mitigation in terms of making the vaccine program safer? How do we have all these vaccines? How do we know we can vaccinate pregnant women? We know because of years and years and years of safety data. Before a vaccine has ever been injected into a pregnant woman, it's probably been tested for decades before we try it in a pregnant woman.
1:14:06.0 DM: We would never, out-of-the-box, take a brand new technology that's never been tested before, ever. And we know that the vaccine technology produces the dangerous spike protein. It produced the Wuhan spike protein, the spicule on the ball of the virus itself, which damages blood vessels and causes blood clotting, and all of them do. We would never unleash that into a pregnant woman's body. Americans have to understand something is very wrong. What's going on? What's going on now in the world? These are examples, are clear-cut examples of wrongdoing that is at such a high level, the groupthink is in the wrong direction in such a consistent and overwhelming way that people are being harmed in an extraordinary fashion.
[pause]
1:15:05.2 DM: Well, when I published the first paper in the American Journal of Medicine, taught doctors how to treat COVID-19. Now, it could have been somebody else. If Dr. Zelenko had the publication power, he could have done it, or Dr. Procter could have done it, or Dr. Didier Raoult could have done it, or Brian Tyson or George Fareed. It turned out that I was the person who had sufficient academic authority to do this. And I have authority, I take complete responsibility for doing this. I did it uniquely. The only person in the world to do this.
1:15:40.0 DM: Others actually may have been trying, and those papers may have been suppressed by editors, they probably were. 'Cause we found suppression of early treatment literature all over. It became impossible to publish papers. It was really hard. I may have just been the strongest and the most courageous doctor in the world to do that, but I did it, and the feedback I was getting was tremendous. It's like, "Of course, this makes sense. I'm so glad this got into the literature." It came out in electronic print in August, and then it came into hard print in January. When it hit January and it landed in all the medical libraries in the world, that's when things really heated up.
Feedback to his paper - do not try treating, we do not have published studies
1:16:18.0 DM: And I do have to tell you that I got letters to the editor that came in to the American Journal of Medicine, and Joe, Dr. Joe Alpert out of Arizona is the editor, Joe has let every one of those letters come to me for a response. The tenor of the letters is quite interesting, and they've come from Duke University, they've come from McGill, from Monash University in Australia. They've come from Brazil. The tenor of the letters is, "Dr. McCullough, you can't do this. You can't treat COVID-19 patients." And it's the most interesting. My response is, "Doctor, please have courage. Let's do away with therapeutic nihilism. Let's join together and treat COVID-19 patients compassionately to reduce hospitalization and death, and we can do this, and I can do it, and we even have more supportive data."
1:17:13.0 DM: So every time they say, "Oh, this drug doesn't work," and I'll say, "Well, here's five more studies that do. Hydroxychloroquine, we're up to hundreds of studies that shows that it works. Ivermectin, hundreds of studies. Steroids, dozens of studies. Anticoagulants, at least a dozen studies." We are so well supported in the concepts of treating COVID-19 that every time one of these letters comes in, I have a little fun with it because the position of strength is enormous. My thoughts and my positions and my statements, over time, are becoming progressively stronger and progressively more powerful. And the detractors sense that, the feeling of fear. Intellectual fear from my adversaries is palpable. I feel it every day.
1:18:02.0 DM: And when that first paper came out in the American Journal of Medicine, my daughter said, "Daddy, why don't you make a YouTube video?" I said, "Ha! Ha! I don't wanna do social media. That's for kids. I just, I don't have time for this." She taught me how to do it. It was PowerPoint. I literally just recorded my face down the lower corner. I wore a tie, four slides. Said, and listen to this, it's Americans, it's Italians. We looked at safety, we looked at efficacy. We looked at all the available data. We think this is the best way to put together the drugs. We had four slides on this, it got up on YouTube, it went absolutely viral, went absolutely viral.
1:18:31.4 DM: And then I got a message. It said, "You violated terms of the community," and it was struck down. Then I got a call from the US Senate. So I told you, I knew something was going on because I've never been called by the White House before, I've never been called by the Senate before. People in Washington were following this. They were stakeholders in Washington, who, in a sense, knew that something is going wrong here, that this viral infection could be treated, but they were waiting for someone in the academic community to step forward and literally say it can be treated. I was the first one to say, "We can treat this! We can do this!" It's very important to be able to make this statement, we can do it. Based on what? Based on my judgement. Based on my judgment, supported by the available science, but more importantly, based on my judgment.
He and his wife got COVID-19 in October
1:19:20.2 DM: And so I ended up contracting COVID-19 myself in October. My wife came home with it, she got sick before I knew I got sick. It got into my lungs. I was in approved protocols. I quickly got into a protocol. It's hard, but I was able to find a protocol. I was on hydroxychloroquine, azithromycin, nutraceutical bundle per the protocol. And later on, I needed steroids 'cause of lung involvement. But I wanted to show America that you could get COVID-19 and have some medical problems, which I do, and be able to get through it without being hospitalized. So on treatment day six, illness day eight, beautiful, sunny day in Dallas, Texas, I went out far away from anybody else, and I went jogging. And I was really short of breath. I'm telling you, I'm a pretty strong runner. I was short of breath 'cause of the COVID involvement in my lungs. But I ran all the way to a park. I made a video in the park, and then I made it all the way home. And I had fun with it.
early treatment doctors started to become scrubbed
1:20:20.0 DM: In fact, I played that Eminem music that said... The Recovery video, if any of you watch Eminem, and I said, "I'm not afraid." And I just... Video of myself, I was, "I'm not afraid of COVID-19," video. That video was struck down and then ultimately had to get restored. I said, "Wait a minute, YouTube is playing a role here, in addition to all the other stakeholders in suppressing any early treatment." In fact, the early treatment doctors started to become scrubbed from Twitter, from YouTube, from social media. And then ultimately, YouTube came out with a very clear message. They said, "Listen, we are only gonna have information that is in line with the CDC, NIH and FDA, which state, 'Do nothing,' and everything else is gonna be considered misleading, and we're making the judgment. It's our call on what's misleading and what's not, but if it's... " It's pretty easy to be in line with the CDC, NIH and FDA because they say to do nothing.
1:21:20.1 DM: So if the social media platform is to do nothing for early treatment and suppress early treatment, which it is, the major media is to suppress early treatment. So I still go back and say, "Who's responsible?" I'd say the government agencies. In this period of crisis, if we're gonna revert to our government agencies and our task force, and if our presidents can't be wise enough to even choose doctors who have ever even seen a patient and know how to treat it, if they're not wise enough to pick doctors who can treat COVID-19, we'll never have agencies that say, "We can treat COVID-19," and if we don't have agencies to do that, then nothing else is gonna follow. If the doctors and people we pick have never seen COVID-19, they're scared of it, they don't know how to treat it, and the only thing they can comment on is wearing masks and social distancing and vaccination, that's all that America's gonna have.
America has offered nothing to the sick person.
1:22:13.6 DM: So America's response to COVID-19, the official response has basically been to well people. Wear masks and be vaccinated, and America has offered nothing to the sick person. When I get in the hospital, we haven't seen much feature on that. The drugs are pretty weak, remdesivir, convalescent plasma, tocilizumab, steroids, anticoagulants, you don't hear much about it and it's honestly too late. Recently, a Harvard group, the Stop COVID Group, had published those sick enough to get in the ICU the 28-day mortality is 38%. Unacceptably high. Going into a hospital is a nightmare. I get desperate calls from all over the United States. Thank goodness for the major telemedicine and regional telemedicine networks that basically have taken over. They're the real heroes of the COVID-19 pandemic. Hospitals are empty now. Hospitals here in Dallas used to have 200, 300 patients at a time. Now, they've got 10, five. The other day in Texas, we hit zero deaths, zero.
1:23:17.4 DM: So early treatment is gonna be one of the great, great stories that historians, and they'll reach out to Ben Marble, who started MyFreeDoctor.com. Ben Marble, that whole telemedicine is run strictly by charity. People donate money, and they get patients their drugs, and they prescribe hydroxychloroquine, ivermectin, steroids and other drugs, and put them into combination, they follow protocols. Terrific! They're seeing thousands of patients by telemedicine every day. So Americans are getting treated. And so the word is out, people talk to each other.
Early treatment without hospitals
1:23:48.9 DM: Americans, it's interesting. They understand that the media and our agencies are not leveling with them. They understand that. I did a seminar early on because I had treated a very prominent African-American minister here in Dallas. And him and his wife were sick, he didn't tell me about his wife, and she was testing negative, she wasn't a patient of mine. He got what's called sequence multidrug therapy. He got really sick. He's got heart failure, diabetes, emphysema, obesity, kidney disease; survives at home sick for about 10 days. I'm not saying the drug therapy's perfect, but I saved him from being hospitalized or dying. His wife, no treatment. Hospitalized, diagnosed late, was in the hospital for five weeks. Came home on oxygen, the virus ravaged her lungs. It was awful! They had the same illness. And so he became active and he said, "Dr. McCullough, can you do a webinar for African-American churches nationwide?" I did a webinar and I presented my approach. And you know what the comments were? They said, "Dr. McCullough, we knew the government was lying to us. We knew this was treatable. We knew it all along." People know this.
[pause]
international Dr. group called C-19
1:25:06.7 DM: It's the individual finance way. There are practices that I've come on. I've gotten calls in Dallas, "Dr. McCullough, can you share your protocols? We wanna do this." The treating doctors really have interdigitated, and we informally called, formed a group called C-19, where we get about four to five email updates a day of really critical updates on treatment. It is international. We have former heads of state involved in C-19. We have Nobel prize winners involved in C-19, hundreds and hundreds of American doctors. There now is a published list of treating doctors, and I assist 250 across all 50 states. Texas has 35 of them.
- c19study.com/d Summary of Vitamin D and COVID studies (the following is updated automatically)
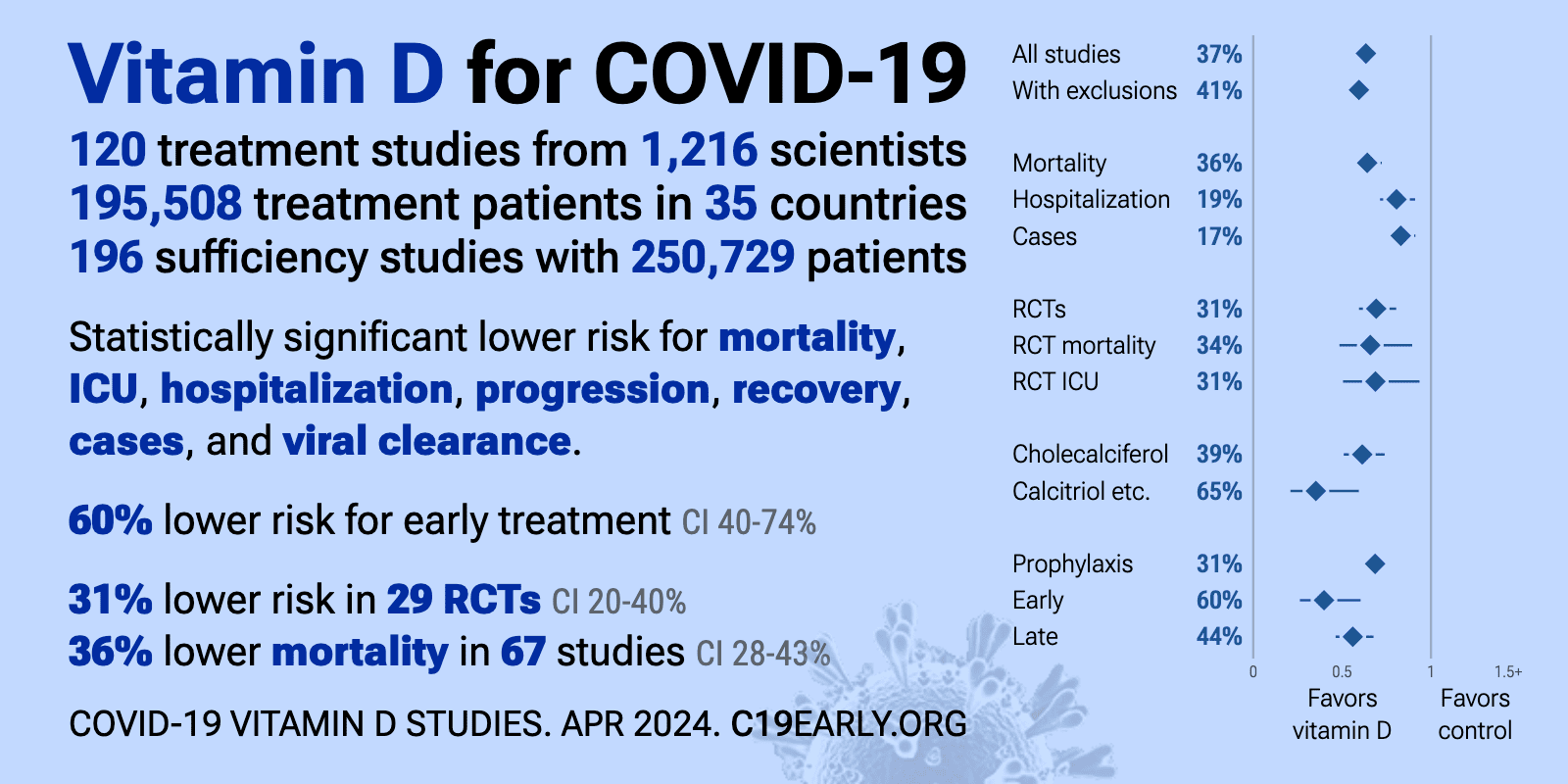
1:25:48.1 DM: So Americans are finding their way, despite suppression of early treatment. It's one of the great stories. And I'll never forget when I testified in the Texas Senate on March 10th, myself and Dr. Richard Urso, another leading early treating doctor in Houston. The Chairwoman of the committee at one of the side conversations said, "Yeah, my husband got COVID-19, and he got really sick, and I'm so glad he got early treatment. We found a doctor that was willing to prescribe ivermectin and the other drugs." And I didn't throw out the zinger in front of the Texas media.
1:26:25.0 DM: But I felt like saying, "You know, do you have to be a chairperson of the Department of Health and Human Services to get some treatment? What about these poor people in South Dallas, in San Antonio, in Houston? What about people who are not so privileged? Do you know that 85% of some of our patients hospitalized here are Black or Hispanic? Who's helping them out?" We should be having early treatment centers. They've been denied treatment. It's heartbreaking. Hispanics and African Americans have double the mortality of Caucasians.
[pause]
Combination therapy works, rarely wil a single drug work
1:27:07.4 DM: We have actually a law in America, it's called the 21st Century Cures Act, and what this says is that the FDA and doctors and others trying to decide on treatment, evaluate the totality of information, including that little anecdote about your mom and the caretaker, as well as case series, large prospective cohort studies, retrospective cohort studies, hospital studies, outpatient studies, and then large prospective randomized double-blind placebo-controlled trials, but any virus, single drugs themselves are very difficult to prove. If we required that for HIV, we'd have no treatment. HIV, we quickly realized we need three or four or five drugs. Everyone understands this. With COVID-19, I never thought a single drug was gonna work. Hydroxychloroquine? No, not alone, but in combination. And it was that thinking, it takes kind of superior thinking that somehow doctors just lost their ability to think. Think a cancer doctor would say, "Oh, there's one pill that cures cancer"? Never. It's always combination cancer therapy.
1:28:10.8 DM: So with hydroxychloroquine, we're now at the stage, obviously, we have hundreds and hundreds of trials. We even have large randomized trials. I've published Dr. Joe Ladapo, only prospective randomized controlled trials show benefit. So at every level, we meet the evidence grade to use hydroxychloroquine. At every level, we meet the evidence grade to use Ivermectin, not so much evidence, but good enough in the monoclonal antibodies. We have the same for steroids. The biggest and best trial in all of COVID-19 is COLCORONA.
[1:28:42.0] I mentioned in the culture scene, shockingly, COLCORONA, the best trial, 4000 patients, double-blind randomized placebo-controlled trial, the best quality that exists, rejected by New England Journal of Medicine, rejected by JAMA, rejected by Lancet.
1:28:58.0 DM: There is a global suppression on any early treatment. I want the listeners to understand how global this is. If we were to go north into Canada, doctors are threatened that their licenses will be examined or taken away if they attempt to treat an outpatient with COVID-19. They are told this in Canada. In Northern EU, the same is true. Dr. Didier Raoult, who was trying to innovate with hydroxychloroquine and azithromycin in France
Drs. being penalized for prescribing treatments
[1:29:30.3] in period times has been under degrees of threat of arrest or partial arrest or house arrest, almost as if we're back in the Dark Ages. In Australia, in April, they put on the books in Queensland, Australia. A doctor who tries to help a patient with hydroxychloroquine could be penalized up unto the point of going into jail for six months for helping. South Africa, they put some doctors in jail for trying to help patients with Ivermectin.
1:30:00.6 DM: Listen, the powers that are out there that wanna suppress early treatment and cause as much fear, suffering, hospitalization and death are not by happenstance. These are powerful forces that have created such fear among doctors. People are fearful they're gonna lose their careers, their livelihood, their medical license. People are afraid of going to jail in just helping their fellow men get through COVID-19. This is extraordinary. Historians should go look through the course of time.
This is not new - The first Dr. using lung machine for polio was thrown off the staff
1:30:34.9 DM: You know the very first doctor who tried to help a polio patient survive polio with the iron lung machine, which became really a stable ICU device, was thrown off medical staff. Throw him off staff.
[pause]
Book: "COVID-19 and the Global Predators: We Are The Prey",
1:30:58.1 DM: I'd look very carefully at the work building upon other investigative reporters. So Dr. Peter Breggin has a book called "COVID-19 and the Global Predators: We Are The Prey", and it has a living document, he's already pre-released the manuscript and he's releasing updates. Now, he's older and he's kind of worried the story won't get out at his age, but I believe he's up to 900 documents. The whole story is not put together, but it is substantial and shows the interconnections of the stakeholders involved. Dr. Nicholas Wade, who was featured on a recent Tucker Carlson as an investigative reporter, he has assembled quite a story. And then Whitney Webb, who's a young investigative reporter, has published some striking things. All three of these, and as well as many more, are linking two important concepts: The suppression of early treatment, and even probably the soft attenuation of in-hospital treatment, to make the problem worse than what it is, many methods to make the case count look higher than what it is, make the mortality numbers look worse than what they are, many methods to create the reaction out of proportion to the reality, so lockdowns, fears, economic suffering, what have you, all of these things making the pandemic way worse than what it is, okay, to have that occur, more fear, suffering, hospitalization and death, loneliness, lockdown, in order to promote mass vaccination.
1:32:51.4 DM: These two are tightly linked. Mass vaccination at all costs, the world must be mass vaccinated. And human beings on Earth ought to understand at this point in time, what we're seeing is unprecedented. It became known the virus was gonna be amenable to a vaccine somewhere around April, May, and at that point in time, therapy was suppressed, nothing could be published, everything, the fake Lancet paper, squashed treatment, and then prepared the population for vaccination.
Why are we vaccinating pregnancies, why are we vaccinating young health care workers?
1:33:25.9 DM: Once the vaccines come out, they're short-tracked, there's all kinds of enthusiasm regarding it, needles and all the arms, trucks rolling, Americans cheering, and then the mass vaccination program starts off. And then before we know it, we're vaccinating pregnant women. Why are we doing that? That can't be safe. Now we're gonna vaccinate COVID-recovered patients. Wait a minute, they have complete and robust permanent immunity. No one's ever challenged the immunity of a COVID-recovered patient. Why are we vaccinating them? And then it keeps going and going. At first, we vaccinated high-risk people. I didn't really understand vaccinating young healthcare workers because they weren't at risk. There were never any hospital outbreaks in the United States. The only thing that was clear, nursing home workers gave it to nursing home patients. We knew that. So nursing home workers should have been vaccinated, and then may be high-risk people, and we should call it a day.
He had estimated maybe 20 million people would need to be vaccinated,
1:34:16.1 DM: I always estimated maybe 20 million people need to be vaccinated, but that didn't seem to satisfy the vaccine stakeholders, which are Pfizer, Moderna, J&J, AstraZeneca, and any others that come forward, the CDC, the FDA, and the NIH and the White House. Massive vaccine stakeholders. You could throw in Gates Foundation, World Health Organization. You can throw those in as well. Massive stakeholders. And they wanted everybody to be vaccinated without exception. No one will escape the needle. We've actually never had this before. And the vaccine process is extraordinary. There's a consent form, it says, "This is investigational. We don't know if it's gonna work. There's only two months of data. The side effects could be a sore arm all the way to death, and we don't know. Sign here. We need your identifying information, we need a barcode on the vial, we need you identified, and now you're in a database. You're vaccinated." And so this mass vaccination is extraordinarily concerning. We never vaccinate into the middle of a pandemic, never. We've never had an effective vaccine for respiratory virus including influenza; it's only modestly effective.
We knew from the clinical trials that it didn't stop COVID-19
1:35:26.7 DM: We knew from the published data that the attack rates in placebo in the vaccine arms were less than 1%. So we know that the vaccine can have a less than 1% effect in the population. Why would it be any different than the clinical trials? We knew from the clinical trials that it didn't stop COVID-19, so people can get COVID-19 anyway. What would be this incredible drive to vaccinate everybody? And now, all my Lord, now the vaccine within a few months has been completely weaponized. Now travel is related to the vaccine. People can't go to school without the vaccine. People are losing their jobs without the vaccine. Believe me, there is something very, very potent in this vaccine. It should be disturbing to everybody. The word "vaccine" ought to be the most disturbing word that they have seen.
He is pro-vaccine in general - but now 4,000 vaccine-related deaths
when Swine vaccine deaths reached 25, it was stopped
1:36:13.2 DM: Now we have 12-year-old children who are told they can decide on their own whether or not they could take a vaccine. So about 70% of my patients are vaccinated, I'm very pro-vaccine, I've taken all the vaccines myself about 70%, and they are all vaccinated in December, January, and February. But as we sit here today in May, we have over 4,000 vaccine-related deaths, and over 10,000 hospitalizations. The limit to shut down a program is about 25 to 50 deaths. Swine flu in 1976, 25 deaths, they shut down the program, it's not safe. All the vaccines in the United States per year, what AmbuLink has reported in the database is about 200. We're talking about vaccinating, probably 500 million injections. Here in the United States at 100 million people vaccinated, this is far and away the most lethal, toxic biologic agent ever injected into a human body in American history, and it's going strong with no mention of safety by our officials, with wild enthusiasm by our hospitals and hospital administrators, with doctors supporting it. Doctors are saying now they won't see patients in their waiting room without the vaccine.
1:37:28.0 DM: This problem, COVID-19 was actually from the very beginning, that's what Whitney Webb said, she goes, "COVID-19 is actually about the vaccine. It's not about the virus, it's about the vaccine."
[pause]
Marked in a database - but not if have nautral immunity?
1:37:50.4 DM: I think it's about what the vaccine means. And Whitney Webb gets credit for this back in April, she said, "A-ha, I figured this out. This is what globalists have been waiting for. They've been waiting for a way of marking people, that you getting a vaccine, you're marked in a database, and this can be used for trade, for commerce, for behavior modification, all different purposes. And you've seen it right here in Dallas, they've announced you can't go to a Dallas Mavericks game unless you're vaccinated. You've had people say, "Listen, you have passports." You had colleges today announced that they're not gonna give any credit to natural immunity. Every scientist in the world knows that the natural immunity is way better than the vaccine immunity. If it's about COVID, why don't we have COVID-recovered go to the Mavericks games? Why don't we have COVID-recovered people freely go to college? Why do we have to have faulty vaccine immunity be the priority, and have natural immunity not count?
1:38:47.5 DM: See, these types of things make me think that Whitney Webb is correct. This is actually about marking. The vaccine is a way of marking people, it's a way of starting to assert efforts to create compliance, behavior control. Don't forget, the vaccine is just a starter. Now there's gonna be updates, there's gonna be boosters, they're already prepping people for this, there's gonna be more... The vaccine manufacturers are all linked, they're all uniquely indemnified. What medical product is there indemnification, where something happens to you, you don't have any recourse? A woman gets vaccinated, a pregnant woman, she has no maternal fetal rights, if something happens to her or her baby, she's out of luck. This is extraordinary, what Americans are doing. It's absolutely extraordinary what's being thrust upon us now.
[pause]
1:39:44.1 DM: I think this whole pandemic from the beginning was about the vaccine. So I think all roads lead to the vaccine. And what it means... There are already places in Southeast Asia and Europe, they're laying the groundwork for compulsory vaccination. I mean compulsory, that means somebody pins you down to the ground and puts a needle in you. That's how bad stakeholders want vaccination. Listen, it's not of cost, you don't have to pay for it, it's all provided. There are people or stakeholders, they do want a needle in every arm. This needle in every arm's a very important moniker. Why? Why do you want a needle in arm... Let's take COVID-recovered, can't get the virus, can't receive it, it has nothing new, why would they ever want a needle in the arm of a COVID-recovered patient? Why? Three studies show higher safety events.
If the vaccine was like water ... who wouldn't take it?
1:40:35.6 DM: See, the tension that Americans are feeling right now as they're try and keep their jobs and go to work is they know they can die of the vaccine. That's the problem. If the vaccine was like water and we just got it and no side effects, who wouldn't take it? Say, "I'll comply. They got my social security number anyway in a database. I'm already marked. I'll just get marked." But no, there's something very unique about this vaccine. There's something about injecting something into a body that is so important to stakeholders, that doesn't matter. Kids, 12 years old, told they can make their own decision on this, and it could be their fatal decision? Think about that. North Carolina just passed that. "Oh, kids, 12 years old, can decide on their own." There are over 4000 dead Americans. There's over 10,000 dead people in Europe that die on days one, two and three after the vaccine. Why are we pushing this in a way where people's jobs and their education and their livelihood decide on a decision that's potentially fatal? The tension, you can cut it with a knife. There are parents that say, "Listen, I want my kid to go to college this year, but I don't wanna lose them to the vaccine." They know what's going on. The internet is full of these cases, blood clots, strokes, immediate death.
He had vaccinated many, but "I can no longer recommend it."
- - patients are getting vaccinated to something that doesn't even exist anymore
"It's just like giving everybody a narrow spectrum antibiotic"
1:41:49.6 DM: Now, I'm fortunate, I have not directly lost a patient to the vaccine. I told you, most got vaccinated in January, December, January, February. Based on the safety data now, I can no longer recommend it. I can't recommend it. It's passed all the thresholds to being a safe product. It's not a safe product, none of them are. It's not just Johnson & Johnson, in fact, more of the safety events in the United States have occurred with Moderna and Pfizer. There are now papers written by prominent scientists, calling for a worldwide halt in the program. There are prominent virologists, many of them, including Noble Prize winners, who have said, "Listen, if we've vaccinate people and we create a very narrow incomplete library of immunity, which what the vaccine is, the vaccines are all targeted to the original Wuhan spike protein, which is long gone, that's extinct, patients are getting vaccinated to something that doesn't even exist anymore." That Wuhan spike protein is gone. We're hoping the immunity covers the other variants, but that narrow immunity is a setup. It's just like giving everybody a narrow spectrum antibiotic. If you did that, what would happen? We grow up super bugs.
1:42:52.1 DM: There are warnings out there saying, "Don't do this. Don't vaccinate the entire world. All we're gonna do is set ourselves up for a super bug that's gonna really wipe out populations." So for many reasons, the vaccine... Indiscriminate vaccination is a horrendous idea, it's a horrendous bio-weapon that's been thrust onto the public, and it's gonna cause great personal harm, which it already has, thousands of people lost their lives. I've never lost a direct patient, but I've had my patients lose their family members, lots of them. I've filled out a safety report on a patient who developed blood clots after one of the Pfizer, Moderna vaccine, and I'm telling you, it took half an hour to do it, there was many pages, and each page said, "Warning, federal offense punishable by severe fines and penalties" if I falsify the report. All those thousands of Americans that have died with the vaccine and hospitalizations in the database I think are real, and they are far beyond anything we've ever seen.
1:43:50.9 DM: And as a doctor, and as a public citizen, I am extraordinarily concerned about the vaccine. The vaccine center right down the street here is empty. I drive past it every day. Americans know, they're talking to each other, the vaccine is not safe, and now the effort is the vaccine stakeholders want kids without parental guidance, and now they wanna be in the church. Americans and people worldwide should be extraordinarily alarmed.
[pause]
1:44:25.4 DM: My personal situation, professional situation is a position of strength, and those who have attempted in any way to pressure, coerce, or threaten me with reprisal have paid an extraordinary price. And I think that's an important message to get out there. There is a position of strength based on principles, of compassionate care, and of the Hippocratic Oath, and of the fiduciary relationship that a doctor has to a patient, and a prominent doctor has to a population that supersedes all of those other ill intents. And what I say is, bring them on.
Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection
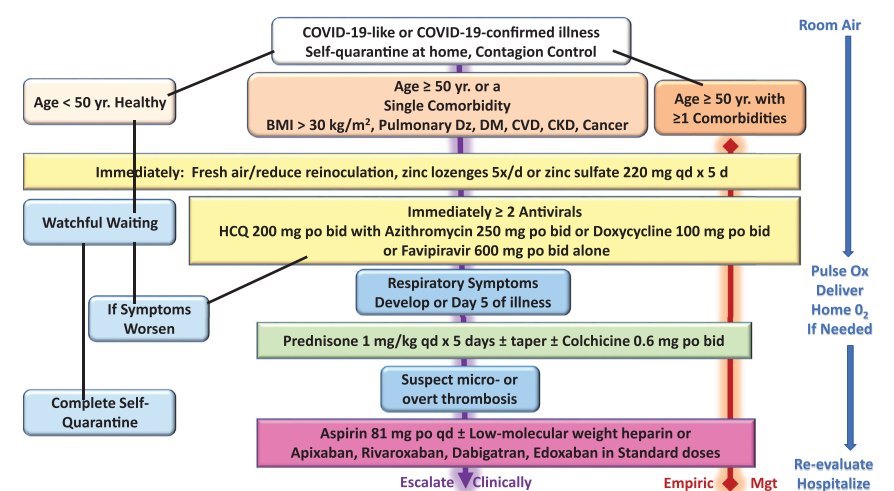
VitaminDWiki
COVID-19 fought by Vitamin D, how much more evidence is needed -May 2021
COVID-19, dark skin, pregnancy - Dr. Grimes, etc. - May 2021
COVID-19 alternative treatments - real-time database C19
1170 vaccinations to prevent 1 severe COVID-19 case , vs 1.2 vaccinations to prevent 1 case of Measles
- As of Sept 6, 2021, the page had: 34 trials, 6 trial results, 23 meta-analyses and reviews, 63 observations, 35 recommendations, 55 associations, 89 speculations, 45 videos see related: Governments, HealthProblems, Hospitals, Dark Skins, 26 risk factors are ALL associated with low Vit D, Recent Virus pages Fight COVID-19 with 50K Vit D weekly Vaccines
Additional ways to prevent COVID-19
COVID-19 risks reduced by Vitamin D, Magnesium, Zinc, Resveratrol, Omega-3, etc. (auto-updated)
Ivermectin
Ivermectin and COVID-19
Vaccines
Many problems with Pfizer COVID-19 vaccine – Nov 9, 2020
Vaccine trials excluded pregnancies, but it is OK to be vaccinated while pregnant
329 COVID-19 vaccine deaths reported to CDC in a month – Jan 22, 2021
Vaccinations resulted in increased office visits for children 16 months later - Nov 2020
10X reactions to flu vaccine when vitamin D deficient
COVID-19 vaccines look good in the short term, but probably not good for the long term
COVID-19 cases increased in 26 countries soon after vaccinations - April, May 2021
Vaccination publications in VitaminDWiki 70 publications as of June 2021
Variants
Reasons why the virus might mutate and become immune to the COVID-19 vaccine – Nov 2020
Worrisome New Evidence That Vaccines Are Less Effective Against Variants - March 2021
Virus videos or books
- Immune system - great 11-minute animated video - Aug 2021
- In-home testing of viral load, etc. Dr. Topol interview with transcript – Aug 11, 2021
- Initial efficacy of vaccines against COVID-Delta - July 20, 2021
- COVID-19 doctors not allowed to use treatments that work - Dr McCullough Video and transcript May 2021
- Vitamin D fights many health symptoms, including COVID-19: Dr. Mahtani video and transcript - April 2021
- COVID public health messages 1, 2, and 3 should be - vitamin d vitamin d, vitamin d (video and transcript) - Mar 5, 2021
- COVID-19 fought by Vitamin D or Heat - Drs Seheult and Patrick video - March 3, 2021
- Vitamin D Deficiency and Covid-19: Book by Drs Anderson and Grimes - July 2020
- Vitamin D and COVID-19 webinar - Feb 24, 2021
- Low-cost Ivermectin and Vitamin D fight COVID-19 – Marik video 1 hr – Feb 18, 2021
- Vitamin D and COVID-19: 1 hour simple video - Jan 31, 2021
- Vitamin D helps the immune system fight COVID-19 – video Jan 21, 2021
- Vitamin D, COVID - Campbell and Davis (Video with transcript) - Jan 18, 2021
- COVID 19 Video - Drs. Seheult and Campbell : Lessons Learned and a Look Ahead - Jan 4
- COVID-19 Vitamin D: Overview by Dr. in Sri Lanka (Video and transcript) - Dec 8, 2020
- COVID-19 Vitamin D: Overview of Evidence by Dr. Seheult (Video and transcript) - Dec 10, 2020
- Vitamin D and COVID-19: Video and PDF by Dr. Grant (includes recommendations)- Nov 25, 2020
- Vitamin D and COVID-19 - observational studies found it helps, never hurts - Campbell Oct 31, 2020
- Can vitamin D fight COVID-19 - interview of Dr. Matthews Oct 2020
- COVID-19 and high-dose Vitamin D - Video interview of Dr. Coimbra - May 2020
- COVID-19 prompts awareness of deficiencies of Vitamin D, C and Magnesium - April 6 2020
Mercola interviewed McCullough: video and transcript (before July 3, 2021)
Mercola video
Download the TRANSCRIPT from VitaminDWiki
McCullough has weekly podcasts
https://americaoutloud.com/the-mccullough-report/
- Without Protection from Pharmaceutical Laws, Vaccines Will Do More Harm - July 5
- Regulation of COVID-19 Vaccines; Who is in Control? - June 23
- Gambling on Biotechnology on the Slope of a Pandemic - June 7
Presentation at Commonwealth Club in SF, July 14, 2021
Early Treatment of COVID-19 and An Update on Vaccine Safety
Rebutal
Vaccines are a safer alternative for acquiring immunity compared to natural infection and COVID-19 survivors benefit from getting vaccinated, contrary to claims by Peter McCullough June 4, 2021 Claim 1 (Inaccurate):, # 2 (Misleading):, # 3 (Inaccurate and Misleading):, # 4 (Misleading and Unsupported):. #5 (Inaccurate): ,# 6 (Unsupported):
Web
Short URL = https://is.gd/mcc521
